Your runner's high isn't endorphins
Ask most people what causes the warm glow after a good run and they will tell you endorphins. Even well established healthcare professionals will. Endorphins are the body's own opioid chemicals, and morphine only works because it mimics them, in exactly the same way that the THC in cannabis only has an effect because it mimics the body's own cannabinoids.
But the molecules doing most of the work after that run belong to a system most people have never heard of, even though every one of us is running it every second of every day. It is the same system that responds to the fats and dietary fibre on your plate. Diet and exercise, two things we usually file in separate boxes, turn out to be talking to the same receptors.
That system is the endocannabinoid system, or ECS.
The body's thermostat
The ECS is a network of receptors (mainly CB1 and CB2), the signalling molecules that activate them, and the enzymes that build and break those molecules down. Its job, broadly, is balance. It helps regulate mood, pain, appetite, sleep, inflammation and stress, nudging things back towards a stable middle when they drift.
The two best understood signalling molecules are anandamide (named after the Sanskrit word for bliss) and 2-AG. Crucially, your body does not keep these in storage. It makes them on demand, from fat.
Why the endorphin theory failed
Endorphins are real and they do rise with exercise. The problem is simple plumbing. Endorphins are too large to cross the blood-brain barrier, so the ones circulating in your blood after a run cannot be the thing changing how your brain feels. That crack in the theory is what sent researchers looking elsewhere in the first place.
Anandamide can cross. Being a fat-soluble molecule, it slips into the brain readily. The brain is the fattiest organ in the body, and fat-soluble molecules pass into it with ease.
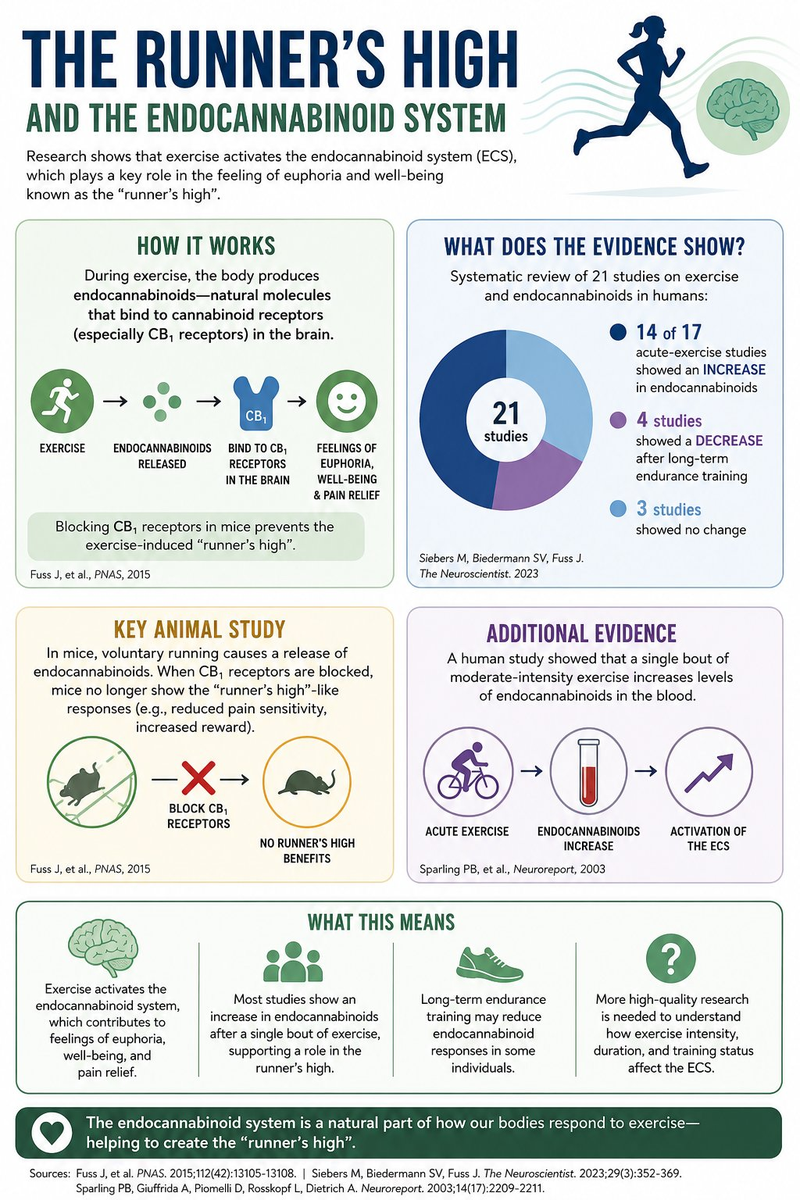
The human evidence is more telling than the plumbing alone. When volunteers are given naltrexone, a drug that blocks opioid receptors, they still feel the euphoria and the drop in anxiety after exercise. If endorphins were the cause, switching off their receptors should switch off the high. It does not. The 2015 mouse study then confirmed it: block the cannabinoid receptors and the calming, pain-dulling effects of running vanish, while blocking the opioid receptors leaves them largely intact. Add the human systematic review, in which 14 of 17 acute-exercise studies found a rise in endocannabinoids, and the bliss molecule, not the endorphin, becomes the better candidate for the runner's high.
The twist nobody mentions
Here is the part that surprised me. The same review found that long-term endurance training appears to push endocannabinoid levels in the opposite direction. Four studies reported a decrease after sustained chronic training.
We do not yet fully understand what that downregulation means, though it may be the system recalibrating to a new normal. The useful takeaway is that the acute hit from a single session is a different beast from the long-term adaptation, and that more is not always better.
Now the bit on your plate
Your endocannabinoids are built from polyunsaturated fats, and you cannot make those fats from nothing. They come from food.
Anandamide and 2-AG are both manufactured from arachidonic acid, an omega-6 fat. Omega-3 fats (the EPA and DHA in oily fish) compete for the same machinery and shift production towards their own, gentler, anti-inflammatory versions, such as DHEA and EPEA. Fibre plays its own part. When gut bacteria ferment it, they produce short-chain fatty acids such as butyrate that feed into the same anti-inflammatory signalling.
This is where the modern diet gets interesting. We eat far more omega-6 than our ancestors did, largely through industrial oils and the changed fat profile of intensively reared animals. An ECS chronically pushed by a flood of omega-6 building blocks behaves differently from one fed a more balanced ratio, and sustained overactivity of the system is linked in the literature to the inflammatory, metabolic picture we see in obesity.
So the omega-6 to omega-3 ratio is not just an abstract nutrition number. It is, quite literally, the raw material supply for the molecules behind your mood, your appetite signalling and your post-exercise calm.
The practical synthesis
You do not need to track endocannabinoid levels to act on this. Two unglamorous things do most of the work.
Move regularly, in a way you will actually keep up. The acute boost is real and it is one of the cleanest, cheapest interventions in medicine.
Mind your fat ratio. More oily fish, fewer industrial omega-6 oils. You are adjusting the supply chain for a signalling system that touches almost everything.
The ECS sits quietly at the junction of how we move and what we eat. We tend to treat diet and exercise as separate projects. Your endocannabinoid system has never seen it that way.
References
1. Fuss J, et al. A runner's high depends on cannabinoid receptors in mice. PNAS. 2015;112(42):13105-13108.
2. Siebers M, Biedermann SV, Fuss J. Do Endocannabinoids Cause the Runner's High? Evidence and Open Questions. The Neuroscientist. 2023;29(3):352-369.
3. Sparling PB, Giuffrida A, Piomelli D, Rosskopf L, Dietrich A. Exercise activates the endocannabinoid system. Neuroreport. 2003;14(17):2209-2211.
4. Banni S, Di Marzo V. Effect of dietary fat on endocannabinoids and related mediators: consequences on energy homeostasis, inflammation and mood. Molecular Nutrition & Food Research. 2010;54(1):82-92.
5. Borsini A, et al. The dietary ligands, omega-3 fatty acid endocannabinoids and short-chain fatty acids, prevent cytokine-induced reduction of human hippocampal neurogenesis. Molecular Psychiatry. 2025.
Comments & discussion
I welcome discussion on everything I write here. Medicine is rarely black and white, and botanical medicine shows even greater variance than most fields. I am genuinely open to other opinions and perspectives, and I read every comment.
Comments are approved before they appear, so there may be a short delay. Frank discussion of drugs, drug use, and differing clinical views is welcome. Hateful or abusive comments are not.